


 What Is Female Sterilization?
What Is Female Sterilization?
- Permanent contraception for women who will not want more children.
- The 2 surgical approaches most often used:
– Minilaparotomy involves making a small incision in the abdomen. The fallopian tubes are brought to the incision to be cut or blocked.
– Laparoscopy involves inserting a long thin tube with a lens in it into the abdomen through a small incision. This laparoscope enables the doctor to see and block or cut the fallopian tubes in the abdomen.
- Also called tubal sterilization, tubal ligation, voluntary surgical contraception, tubectomy, bi-tubal ligation, tying the tubes, minilap, and “the operation.”
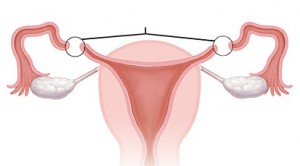
- Works because the fallopian tubes are blocked or cut. Eggs released from the ovaries cannot move down the tubes, and so they do not meet sperm.
One of the most effective methods but carries a small risk of failure:
- Less than 1 pregnancy per 100 women over the first year after having the sterilization procedure (5 per 1,000). This means that 995 of every 1,000 women relying on female sterilization will not become pregnant.
- A small risk of pregnancy remains beyond the first year of use and until the woman reaches menopause.
– Over 10 years of use: About 2 pregnancies per 100 women (18 to 19 per 1,000 women).
- Effectiveness varies slightly depending on how the tubes are blocked, but pregnancy rates are low with all techniques. One of the most effective techniques is cutting and tying the cut ends of the fallopian tubes after childbirth (postpartum tubal ligation).
Fertility does not return because sterilization generally cannot be stopped or reversed. The procedure is intended to be permanent. Reversal surgery is difficult, expensive, and not available in most areas. When performed, reversal surgery often does not lead to pregnancy
Protection against sexually transmitted infections (STIs): None
Side Effects
None
Known Health Benefits
Helps protect against кisks of pregnancy, and pelvic inflammatory disease (PID)
May help protect against ovarian cancer
Known Health Risks
Uncommon to extremely rare: complications of surgery and anesthesia
Complications of Surgery
Uncommon to extremely rare:
- Female sterilization is a safe method of contraception. It requires surgery and anesthesia, however, which carry some risks such as infection or abscess of the wound. Serious complications are uncommon. Death, due to the procedure or anesthesia, is extremely rare.
The risk of complications with local anesthesia is significantly lower than with general anesthesia. Complications can be kept to a minimum if appropriate techniques are used and if the procedure is performed in an appropriate setting.
Safe for All Women
With proper counseling and informed consent, any woman can have female sterilization safely, including women who:
- Have no children or few children
- Are not married
- Do not have husband’s permission
- Are young
- Just gave birth (within the last 7 days)
- Are breastfeeding
- Are infected with HIV, whether or not on antiretroviral therapy
In some of these situations, especially careful counseling is important to make sure the woman will not regret her decision.
Women can have female sterilization:
- Without any blood tests or routine laboratory tests
- Without cervical cancer screening
- Even when a woman is not having monthly bleeding at the time, if it is reasonably certain she is not pregnant
Female sterilization:
- Does not make women weak.
- Does not cause lasting pain in back, uterus, or abdomen.
- Does not remove a woman’s uterus or lead to a need to have it removed.
- Does not cause hormonal imbalances.
- Does not cause heavier bleeding or irregular bleeding or otherwise change women’s menstrual cycles.
- Does not cause any changes in weight, appetite, or appearance.
- Does not change women’s sexual behavior or sex drive.
- Substantially reduces the risk of ectopic pregnancy.
Problems Reported as Complications:
- Infection at the incision site (redness, heat, pain, pus)
- Abscess (a pocket of pus under the skin caused by infection)
- Severe pain in lower abdomen (suspected ectopic pregnancy)
- Suspected pregnancy
Contact your doctor if you have any of the problems listed above.
1. Will sterilization change a woman’s monthly bleeding or make monthly bleeding stop?
No. Most research finds no major changes in bleeding patterns after female sterilization. If a woman was using a hormonal method or IUD before sterilization, her bleeding pattern will return to the way it was before she used these methods. For example, women switching from combined oral contraceptives to female sterilization may notice heavier bleeding as their monthly bleeding returns to usual patterns. Note, however, that a woman’s monthly bleeding usually becomes less regular as she approaches menopause.
2. Will sterilization make a woman lose her sexual desire? Will it make her fat?
No. After sterilization a woman will look and feel the same as before. She can have sex the same as before. She may find that she enjoys sex more because she does not have to worry about getting pregnant. She will not gain weight because of the sterilization procedure.
3. Should sterilization be offered only to women who have had a certain number of children, who have reached a certain age, or who are married?
No. There is no justification for denying sterilization to a woman just because of her age, the number of her living children, or her marital status. Health care providers must not impose rigid rules about age, number of children, age of last child, or marital status. Each woman must be allowed to decide for herself whether or not she will want more children and whether or not to have sterilization.
4. Is it not easier for the woman and the health care provider to use general anesthesia? Why use local anesthesia?
Local anesthesia is safer. General anesthesia is more risky than the sterilization procedure itself. Correct use of local anesthesia removes the single greatest source of risk in female sterilization procedures—general anesthesia. Also, after general anesthesia, women usually feel nauseous. This does not happen as often after local anesthesia. When using local anesthesia with sedation, however, providers must take care not to overdose the woman with the sedative. They also must handle the woman gently and talk with her throughout the procedure. This helps her to stay calm. With many clients, sedatives can be avoided, especially with good counseling and a skilled provider.
5. Does a woman who has had a sterilization procedure ever have to worry about getting pregnant again?
Generally, no. Female sterilization is very effective at preventing pregnancy and is intended to be permanent. It is not 100% effective, however. Women who have been sterilized have a slight risk of becoming pregnant: About 5 of every 1,000 women become pregnant within a year after the procedure. The small risk of pregnancy remains beyond the first year and until the woman reaches menopause.
6. Pregnancy after female sterilization is rare, but why does it happen at all?
Most often it is because the woman was already pregnant at the time of sterilization. In some cases an opening in the fallopian tube develops. Pregnancy also can occur if the provider makes a cut in the wrong place instead of the fallopian tubes.
7. Can sterilization be reversed if the woman decides she wants another child?
Generally, no. Sterilization is intended to be permanent. People who may want more children should choose a different family planning method. Surgery to reverse sterilization is possible for only some women—those who have enough fallopian tube left. Even among these women, reversal often does not lead to pregnancy. The procedure is difficult and expensive, and providers who are able to perform such surgery are hard to find. When pregnancy does occur after reversal, the risk that the pregnancy will be ectopic is greater than usual. Thus, sterilization should be considered irreversible.
8. Is it better for the woman to have female sterilization or the man to have a vasectomy?
Each couple must decide for themselves which method is best for them. Both are very effective, safe, permanent methods for couples who know that they will not want more children. Ideally, a couple should consider both methods. If both are acceptable to the couple, vasectomy would be preferable because it is simpler, safer, easier, and less expensive than female sterilization.
9. Will the female sterilization procedure hurt?
Yes, a little. Women receive local anesthetic to stop pain, and, except in special cases, they remain awake. A woman can feel the health care provider moving her uterus and fallopian tubes. This can be uncomfortable. If a trained anesthetist or anesthesiologist and suitable equipment are available, general anesthesia may be chosen for women who are very frightened of pain. A woman may feel sore and weak for several days or even a few weeks after surgery, but she will soon regain her strength.
10. How can health care providers help a woman decide about female sterilization?
Provide clear, balanced information about female sterilization and other family planning methods, and help a woman think through her decision fully. Thoroughly discuss her feelings about having children and ending her fertility. For example, a provider can help a woman think how she would feel about possible life changes such as a change of partner or a child’s death. .
11. Does female sterilization increase the risk of ectopic pregnancy?
No. On the contrary, female sterilization greatly reduces the risk of ectopic pregnancy. Ectopic pregnancies are very rare among women who have had a sterilization procedure. The rate of ectopic pregnancy among women after female sterilization is 6 per 10,000 women per year. The rate of ectopic pregnancy among women in the United States using no contraceptive method is 65 per 10,000 women per year. On the rare occasions that sterilization fails and pregnancy occurs, 33 of every 100 (1 of every 3) of these pregnancies are ectopic. Thus, most pregnancies after sterilization failure are not ectopic. Still, ectopic pregnancy can be life-threatening, so a provider should be aware that ectopic pregnancy is possible if sterilization fails.
12. Where can female sterilization be performed?
If no pre-existing medical conditions require special arrangements:
- Minilaparotomy can be provided in maternity centers and basic health facilities where surgery can be done. These include both permanent and temporary facilities that can refer the woman to a higher level of care in case of emergency.
- Laparoscopy requires a better equipped center, where the procedure is performed regularly and an anesthetist is available.
13. What are transcervical methods of sterilization?
Transcervical methods involve new ways of reaching the fallopian tubes, through the vagina and uterus. A microcoil, Essure, is already available in some countries. Essure is a spring-like device that a specifically trained clinician using a viewing instrument (hysteroscope) inserts through the vagina into the uterus and then into each fallopian tube. Over the 3 months following the procedure, scar tissue grows into the device. The scar tissue permanently plugs the fallopian tubes so that sperm cannot pass through to fertilize an egg. Essure is unlikely to be introduced in low-resource settings soon, however, because of the high cost and complexity of the viewing instrument required for insertion.
For a family planning consultation:
- Ask your family doctor at your health care facility in your area of residence (see here). WARNING: if you belong to one of the socially vulnerable groups (see here) you can benefit from free contraceptives!
- Ask Youth Friendly Health Centers
- Call the RHTC Hotline (free and confidential call) – 0800-088-08
- Call RHTC – 022355072 / 060903782 / 078306973
- Write to RHTC e-mail – cidsr2012@gmail.com